
Classification of periodontitis
- What are the shortcomings of the current 1999 classification with regards to periodontitis?
- These include substantial overlap and lack of clear pathobiology‐based distinction between the stipulated categories, diagnostic imprecision, and implementation difficulties.
- Which different forms of periodontitis are recognised in the present revised classification system?
- Periodontitis
- Necrotising periodontitis
- Periodontitis as a direct manifestation of systemic diseases.
- Why have “chronic” and “aggressive” periodontitis been taken out the classification?
- There is no evidence for specific pathophysiology that can distinguish between aggressive and chronic periodontitis or provide solid guidance for different types of intervention.
- Research data do not support the notion that aggressive and chronic are different diseases, although there is evidence that multiple factors have a role in what we observe as the phenotype.
- “Chronic” and “aggressive” are now grouped under a single category of “periodontitis” and are further characterised based on a multi-dimensional staging and grading system. A more restrictive definition might be better suited to take advantage of modern methodologies to enhance knowledge on the diagnosis, pathogenesis, and management of periodontitis.
- What do we know about the rates of periodontitis progression?
- On a population basis, the mean rates of periodontitis progression are fairly consistent across studies carried out in different parts of the world.
- In all populations, however, specific subsets in each age group exhibit different levels of periodontitis severity and progression.
- Where was the idea of staging and grading derived from?
- The new classification based on staging and grading was inspired by a system used in oncology that:
- Individualises the diagnosis and the case definition of a periodontitis patient and aligns it to the principles of personalised medicine.
- Takes into account the multifactorial aetiology of the disease, the level of complexity of management, and the risk of disease recurrence or progression, to facilitate optimal care and improve prognosis.
- Which are the main features that identify periodontitis?
- Periodontitis is a chronic multifactorial inflammatory disease associated with bacterial dysbiosis and characterised by progressive destruction of the tooth-supporting structures.
- Its primary features include the loss of periodontal tissue support, manifested through clinical attachment loss and radiographic bone loss, presence of periodontal pocketing and gingival bleeding.
- A patient is a “periodontitis case” if: interdental CAL is detectable at 2 or more non-adjacent teeth and buccal or oral CAL >3 mm with pocketing > 3 mm is detectable at two or more teeth.
- The observed CAL cannot be ascribed to causes other than periodontitis, such as gingival recession of traumatic origin, dental caries extending in the cervical area of the tooth, the presence of CAL on the distal aspect of a second molar and associated with malposition or extraction of a third molar, an endodontic lesion draining through the marginal periodontium and the occurrence of a vertical root fracture.
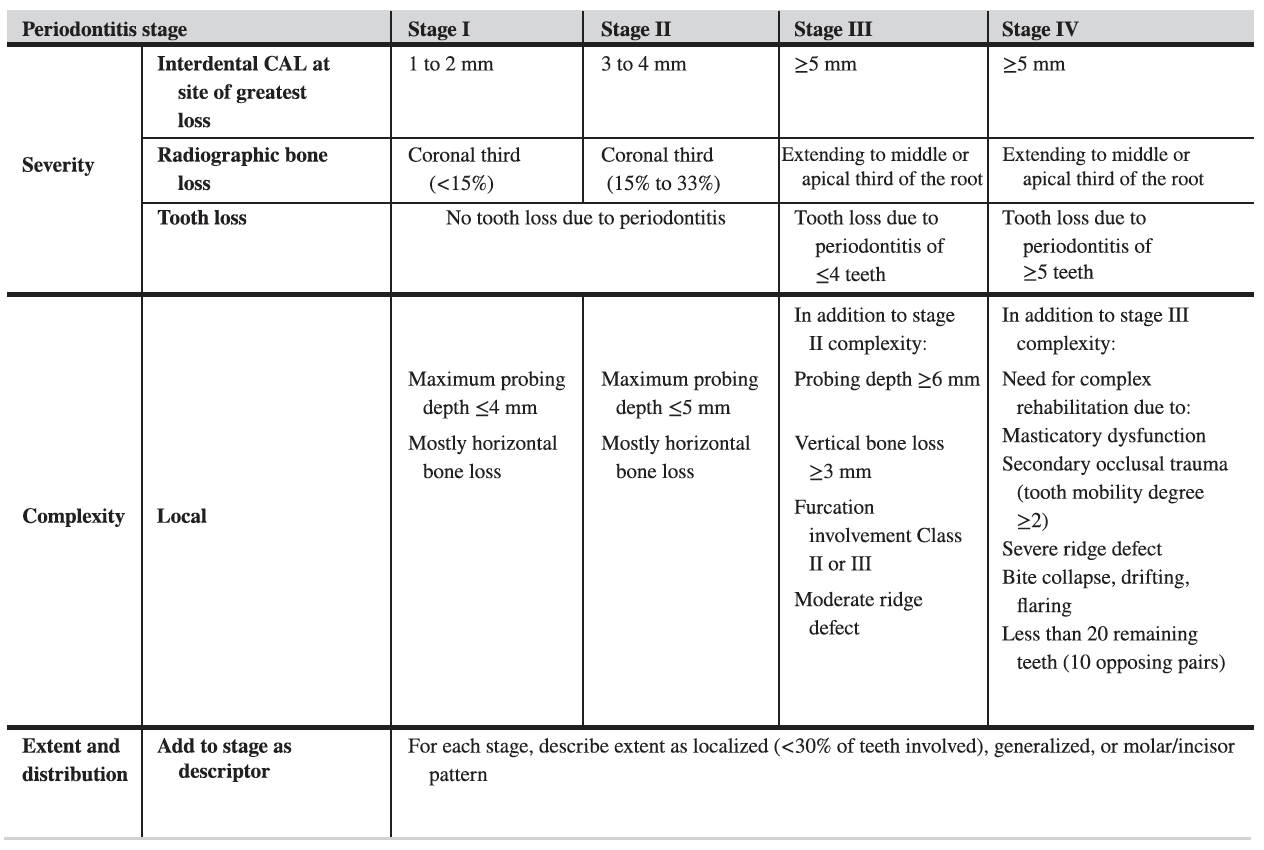
- What does staging involve?
- Staging classifies the severity and extent of current tissue loss, including tooth loss, due to periodontitis.
- Incorporates an assessment of the level of complexity in the long-term management of function and aesthetics of the patient’s dentition.
- When accounting for missing teeth, the patient may not always be able to fully appreciate why a tooth was removed. You may not get an accurate answer by just asking question. However, there is a lot of redundancy in the grid so if you are not sure of the answer then you can approach the staging in another way. Not all the criteria in the grid have to be fulfilled.
- The terms masticatory dysfunction and occlusal trauma have been introduced to ensure the outcome of the disease process is fully understood in terms of function.
- Stage IV has been added to ensure the profession are careful with analysis of advanced cases. It ensures the question of engaging with multidisciplinary treatment is considered. This decision is important for overall success of treatment because in the end we want the patient to have a functional and aesthetically pleasing dentition. Accounting for the fact that the patient needs more advanced management is also useful in terms of communication with the patient.
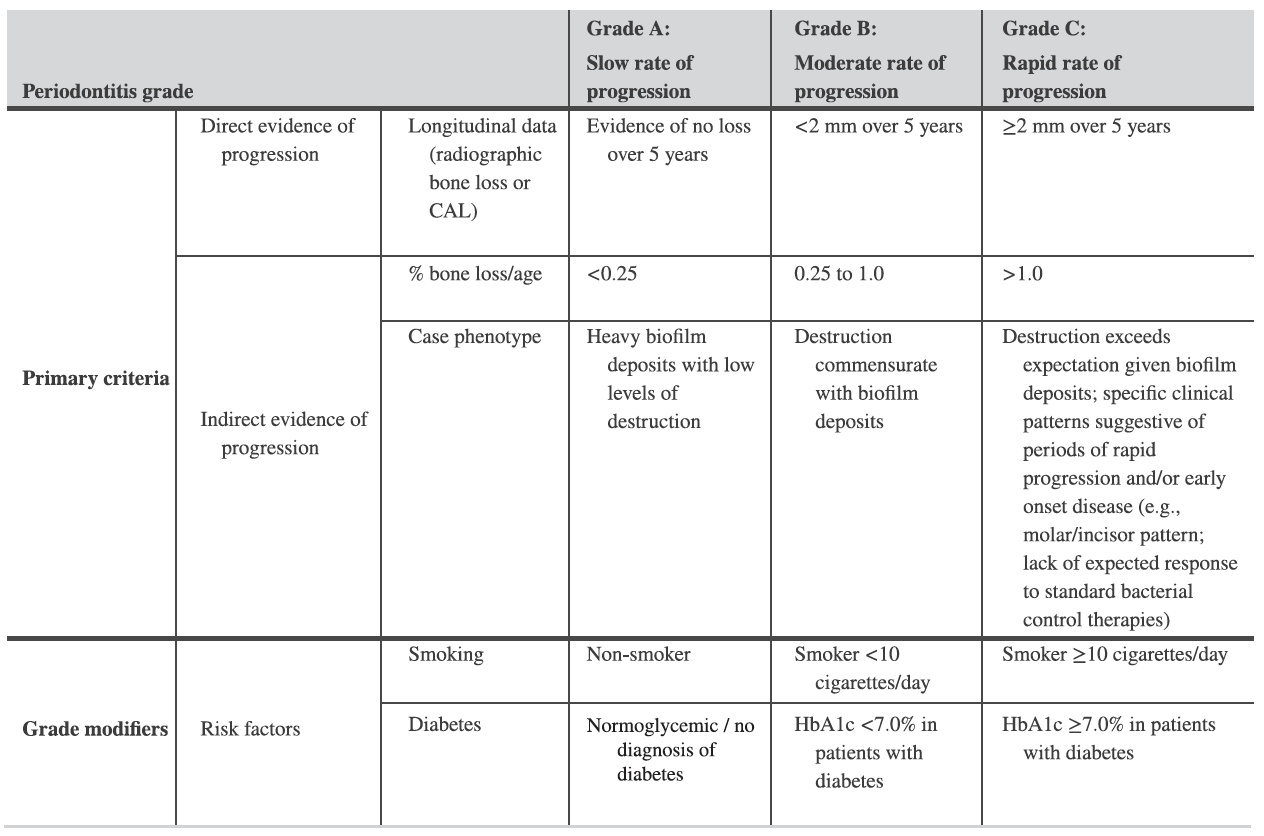
- What does grading involve?
- Grading incorporates 4 additional biological dimensions:
- History-based periodontitis progression.
- Risk of further periodontitis progression.
- Anticipated inferior treatment outcomes.
- Risk that the disease or its treatment may negatively affect the general health of the patient.
- One of the benefits of the new classification is that is accounts of risk factors / “grade modifiers”, specifically smoking and diabetes.
- The grade can be revised after you assess initial treatment responses, compliance, and risk factor control.
- What’s the most practical approach of coming up with your periodontitis classification?
- Step 1: Initial overview of the case – screen full mouth radiographs, full mouth probing depths and missing teeth – distinguish between stage I/II and III/IV. Is it mild/moderate periodontitis or severe/very severe periodontitis?
- Step 2: Determine stage –
- Determine maximum CAL or radiographic bone loss and confirm bone loss pattern (horizontal/angular) – Stages I/II.
- Check for tooth loss due to periodontitis and determine case complexity (full mouth probing depths, furcation involvements, occlusion/function, need for extensive rehabilitation etc.) – Stages III and IV.
- Step 3: Determine grade –
- History/risk of progression/age, risk factors and medical status and systemic inflammatory consideration – default grade B.
- Response to SRP and plaque control and detailed assessments – refine grade.
- Step 4: Treatment plan – if stages I/II then standard periodontal treatment, if stages III/IV then complex and/or multidisciplinary treatment.
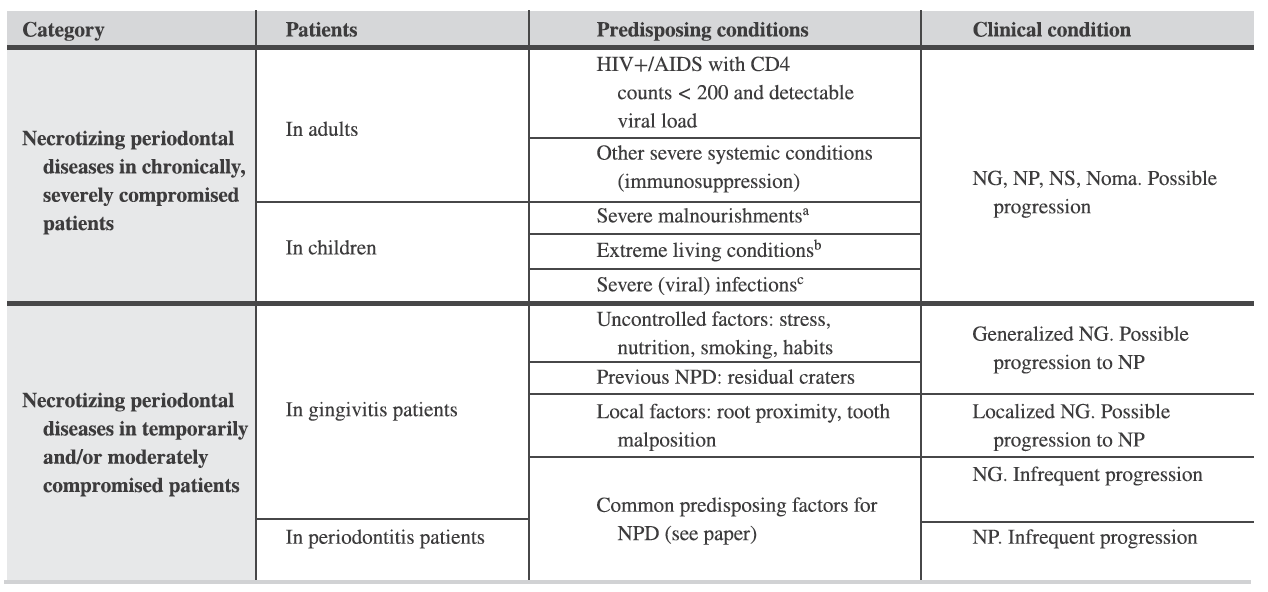
- What does the classification of necrotising periodontal diseases involve?
- These are characterised by three typical clinical features (papilla necrosis, bleeding, and pain) and are associated with host immune response impairments, which should be considered in the classification of these conditions. Other signs/symptoms associated with this condition may include pseudomembrane formation, lymphadenopathy, and fever.
- Host immune response impairments include: chronically, severely compromised patients (e.g., AIDS patients, children suffering from severe malnourishment etc.) or temporarily and/or moderately compromised patients (e.g., in smokers or psycho‐socially stressed adult patients).
- Necrotising periodontal diseases have a distinct pathophysiology. They are characterised by the presence of ulcers within the stratified squamous epithelium and the superficial layer of the gingival connective tissue, surrounded by a non‐specific acute inflammatory infiltrate.
- Categories: nectrotising gingivitis, periodontitis and stomatitis.
- What does “periodontitis as a manifestation of systemic disease” constitute of?
- Periodontitis as a direct manifestation of systemic disease should follow the classification of the primary disease according to the respective International Statistical Classification of Diseases and Related Health Problems (ICD) codes.
- Management of this is still driven by a dysbiotic biofilm i.e. we still focus on plaque control. This is an important tweak from the previous classification.
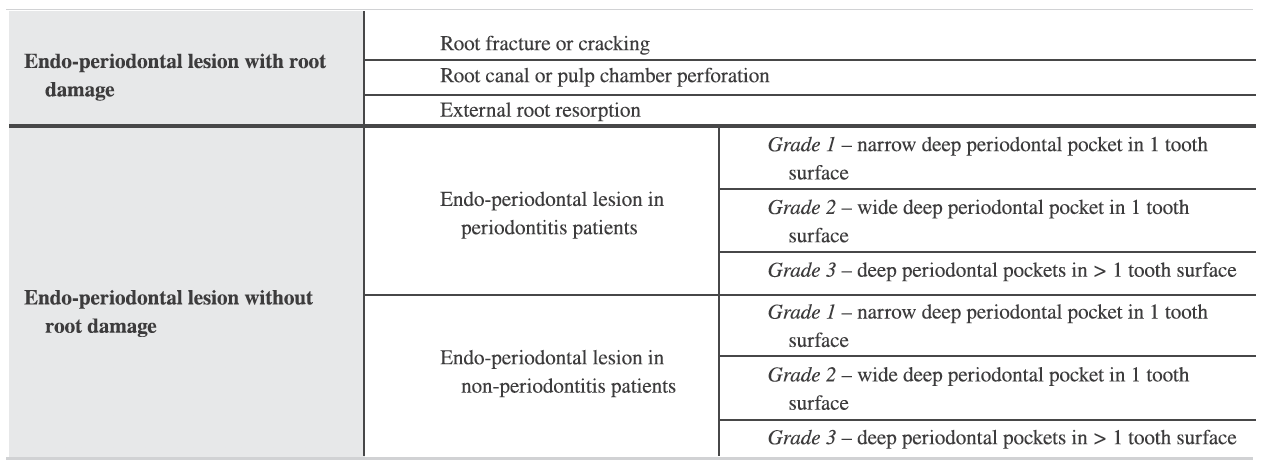
- How are endodontic-periodontal lesions defined?
- Endodontic‐periodontal lesions are defined by a pathological communication between the pulpal and periodontal tissues at a given tooth, occur in either an acute or a chronic form, and should be classified according to signs and symptoms that have direct impact on their prognosis and treatment (i.e., presence or absence of fractures and perforations, and presence or absence of periodontitis).
- An endo‐periodontal lesion is a pathologic communication between the pulpal and periodontal tissues at a given tooth that may occur in an acute or a chronic form. The primary signs associated with this lesion are deep periodontal pockets extending to the root apex and/or negative/altered response to pulp vitality tests. Signs observed in endo‐periodontal lesions associated with traumatic and/or iatrogenic factors may include root perforation, fracture/cracking, or external root resorption. These conditions drastically impair the prognosis of the involved tooth.
- The review did not identify evidence for a distinct pathophysiology between an endo‐periodontal and a periodontal lesion. Nonetheless, the communication between the pulp/root canal system and the periodontium complicates the management of the involved tooth.
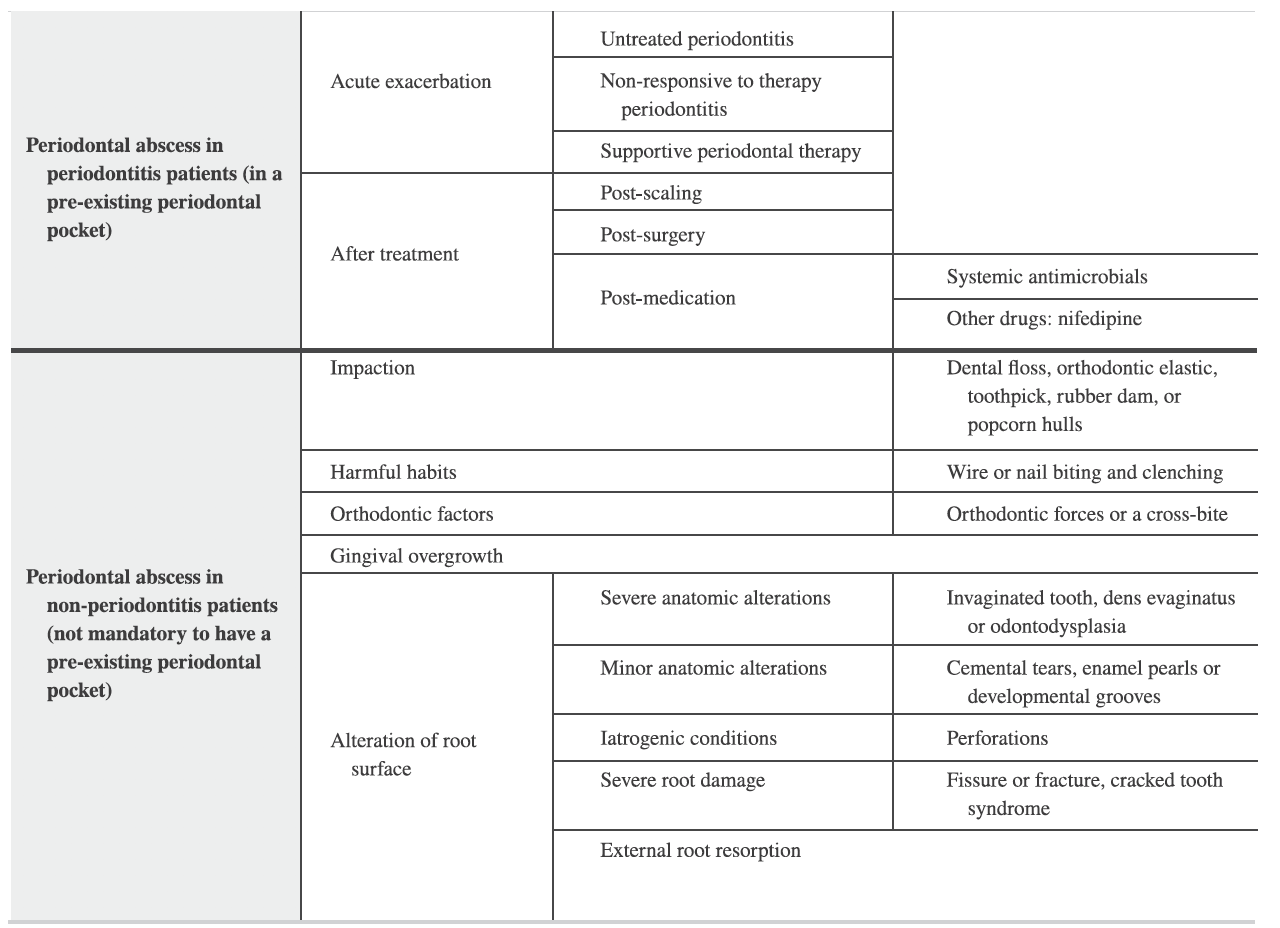
- What about periodontal abscesses?
- Periodontal abscesses most frequently occur in pre‐existing periodontal pockets and should be classified according to their aetiology. They are characterised by localised accumulation of pus within the gingival wall of the periodontal pocket/sulcus, cause rapid tissue destruction which may compromise tooth prognosis, and are associated with risk for systemic dissemination.
- The primary detectable signs/symptoms associated with a periodontal abscess may involve ovoid elevation in the gingiva along the lateral part of the root and bleeding on probing.
- Pathophysiologically of a periodontal abscess differs in that the low pH within an abscess leads to rapid enzymatic disruption of the surrounding connective tissues and, in contrast to a chronic inflammatory lesion, has a greater potential for resolution if quickly managed.
- Final key points to be aware of:
- The new classification has an in-build plan for periodic revisions, without having to change nomenclature.
- You do not have to populate every single cell of the grid before arriving at an assessment of stage and grade.
- Example of how it should appear in your notes: Periodontitis stage II (generalised), grade B.
- You should not be afraid of revising your diagnosis at a later stage.
- Much simpler than what you may gather at your first glance!
Periodontology
Recent post
June 29, 2023
Pink Aesthetics...
Read more
General Dental,Periodontology
June 26, 2022
10 Key Points from EuroPerio10...
Read more
Periodontology,Reena's Notes
June 11, 2021
Working as a hygienist or therapist...
Read more
General Dental,Periodontology



